Domínguez-Rodríguez LM, Dobarro D, Iglesias C, Crespo MG, Raposeiras S, Álvarez J, Barreiro M, Muñoz I, Sánchez A, Íñiguez Á, Zamorano JL. Guideline-directed medical therapy for heart failure in arrhythmia-induced cardiomyopathy with improved left ventricular ejection fraction
Eur J Heart Fail. 2024
"Maintaining RAS inhibitors and beta-blockers is associated with a significantly lower incidence of heart failure relapse in patients with arrhythmia-induced cardiomyopathy and improved left ventricular ejection fraction" - Dr. Luis Manuel Domínguez Rodríguez & Dr. José Luis Zamorano
Summary:
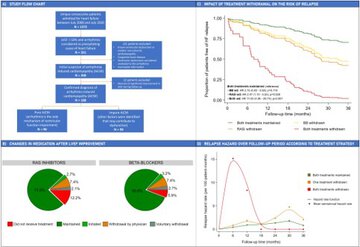
Aims: No study has analyzed the impact of guideline-directed medical therapy in preventing heart failure (HF) relapse in patients with arrhythmia-induced cardiomyopathy (AiCM) following left ventricular ejection fraction (LVEF) improvement.
Methods and results: We analyzed data from a single-center cohort of 200 patients admitted for HF, LVEF <50% and cardiac arrhythmia considered by cardiologists to be the precipitating cause of the episode. The primary endpoint was time-to-HF relapse, defined as the composite of readmission for HF, Emergency Department (ED) visit for HF, or significant decline in LVEF. Changes in medication were recorded and a time-varying multivariate Cox regression was performed. After a median follow-up period of 6.14 years, diagnostic confirmation was achieved in 188 out of the initial 200 patients with suspected AiCM. A total of 89 patients (47.3%) met the primary endpoint. RAS inhibitors (adjusted hazard ratio (HR) 0.50 [0.31-0.81]; p = 0.005) and beta-blockers (adjusted HR 0.48 [0.28-0.81]; p = 0.006) were associated with a lower incidence of relapse. Mineralocorticoid receptor antagonists were associated with a significantly lower incidence of ED visits for HF (adjusted HR 0.38 [0.15-0.95]; p = 0.038), but did not achieve statistical significance for the combined primary endpoint. Antiarrhythmic drugs did not show a significant impact on the primary endpoint.
Conclusion: Maintaining RAS inhibitors and beta-blockers was associated with a significantly lower incidence of relapse in the setting of AiCM with improved LVEF.
Why do you highlight this publication?
The present study analyzes a cohort of 188 patients with confirmed arrhythmia-induced cardiomyopathy (AiCM), one of the largest described in literature for this condition and the one with the longest follow-up period. It is also the first to evaluate the role of neurohormonal therapy in AiCM beyond left ventricular ejection fraction (LVEF) improvement. Our results reinforce that treatment with RAS inhibitors and beta-blockers is associated with a lower risk of heart failure relapse, significantly improves relapse-free survival, and its benefit remains consistent regardless of the type of AiCM (pure or impure) and degree of LVEF improvement (complete or partial). These findings support indefinite maintenance of guideline-directed medical therapy in patients with AiCM and improved LVEF, a clinical scenario where specific evidence and recommendations from clinical practice guidelines are currently lacking.
Publication commented by:
Dr. Luis Manuel Domínguez Rodríguez & Dr. José Luis Zamorano Gómez
CARDIOVASCULAR DISEASES group
IRYCIS