Fernández A, Subiela JD,..., Burgos FJ. Impact of re-transurethral resection of bladder staging on risk stratification of high-grade T1 non-muscle-invasive bladder cancer across European Association of Urology 2021 risk groups
BJU Int. 2026
"Re-TURB findings redefine risk and guide treatment decisions in T1HG NMIBC". - Ana Fernández-Mardomingo & Dr. Fco. Javier Burgos Revilla
Summary:
Objective: To evaluate the prognostic impact of T-stage at re-transurethral resection of bladder (TURB) and its utility for refining risk stratification across European Association of Urology 2021 (EAU21) risk groups in patients with T1 high-grade (HG) non-muscle-invasive bladder cancer (NMIBC) treated with adequate Bacillus Calmette-Guérin (BCG).
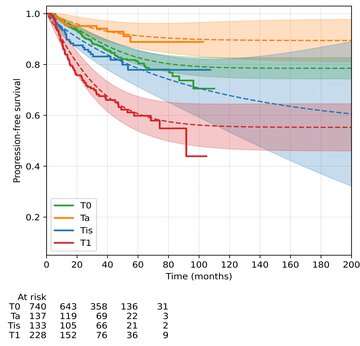
Patients and methods: Retrospective multicentre study including patients with primary or secondary T1HG NMIBC treated with TURB, re-TURB, and adequate BCG between 2007 and 2020 across 28 European academic centres. Patients were stratified according to re-TURB pathological stage (T0, Ta, Tis, T1) and EAU21 risk groups. Kaplan-Meier, Cox regression, and competing-risk methods were used to evaluate recurrence-free survival (RFS), HG-RFS, progression-free survival (PFS), and cancer-specific mortality (CSM). A mixture cure model estimated statistical cure fractions for the overall cohort.
Results: Among 1403 patients, residual disease at re-TURB was identified in 38.8%, including 17.7% with persistent T1. Residual T1 was consistently associated with worse outcomes. Compared with T0/Ta, persistent T1 at re-TURB showed substantially lower 5-year HG-RFS and PFS, with high-grade recurrence in over half of patients and 5-year progression up to 48% in high- and very high-risk groups. The 5-year CSM rose from 6-7% (T0/Ta) to 23% (T1). On multivariable analysis, residual T1 was independently associated with worse HG-RFS (hazard ratio 2.40), PFS (hazard ratio 3.10), and CSM (hazard ratio 3.00). Cure modelling showed lower cure fractions for residual T1 compared with T0/Ta.
Conclusion: Residual T1 at re-TURB is strongly associated with adverse long-term oncological outcomes in BCG-treated T1HG NMIBC and markedly reduces the likelihood of statistical cure. High- and very high-risk patients with persistent T1 represent a biologically adverse subgroup in whom standard BCG may be insufficient.
Why do you highligth this publication?
This study shows that persistent T1 at re-TURB is a strong independent predictor of recurrence, progression, and cancer-specific mortality in BCG-treated T1 High-grade non-muscle-invasive bladder cancer. Importantly, re-TURB pathology refines risk stratification beyond current EAU21 models, identifying subgroups that may benefit from early radical or intensified treatment strategies.
Publication commented by:
Ana Fernández-Mardomingo & Dr. Fco. Javier Burgos Revilla
SURGICAL RESEARCH IN UROLOGY AND RENAL TRASPLANTATION. IRYCIS